|
|
|
Case #10
|
Typical Clinical Presentation:
|
|
A 14-year-old female presented with a 3 months history of increasing pain in her elbow.
|
|
|
|
Characteristic Radiological Findings:
|
|
|

|
-
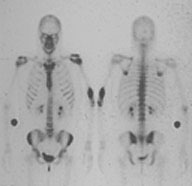
Plain film showed a well circumscribed, "punched-out" lytic, intramedullary lesion in the
distal humeral shaft. There was no sclerotic rim and no periosteal reaction.
|
|
|
|
-
Full skeletal survey showed no other lesions.
|
|
A well defined, "punched-out" appearance, intramedullary location and lack of periosteal
reaction are very common in this lesion.
|
|
|
|
Pathological Findings: :
|
|
|
|
-
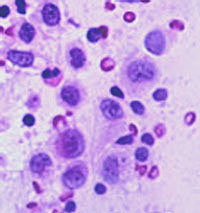
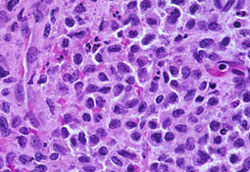
Microscopically, the lesion was composed of several cell types.
The predominant cell population was that of mononuclear, histiocyte-like cells with
indented or grooved nuclei and distinct cytoplasmic borders (Langerhans cells).
No mitoses were seen.
|
|
|
|
-
The lesion also contained multiple eosinophils, mononuclear
inflammatory cells and occasional osteoclast-like, multinucleated giant cells.
|
|
|
Diagnosis: Eosinophilic Granuloma (EG)
|
|
Salient Points::
|
-
Classification of the lesions of Langerhans Cell Histiocytosis is based on the extent of
disease and includes the following three forms:
- eosinophilic granuloma (localized form of disease at single skeletal sites)
- Hand-Schuller-Christian disease (extensive, multifocal, symptomatic disease
with predominantly skeletal involvement)
- Letterer-Siwe disease (aggressive systemic form of disease
that involves multiple organs and systems and leads to functional impairment of the
affected sites).
-
EG commonly occurs in individuals younger than 30 years and has the highest incidence in the first decade of life.
-
Location. Skeletal sites include craniofacial bones, ribs, vertebrae, pelvis, and major long bones such as
femur and humerus. Small bones of the hands and feet are not affected. Extraskeletal lesions most commonly
arise in the lungs and lymph nodes.
-
The Langerhans cells are pathognomonic and clonal. They are characterized by histiocyte-like appearance
and indented or grooved nuclei. Unlike histiocytes, these cells show strong positivity for S-100 and CD1a,
and contain Birbeck granules (rod-shaped and tennis racquet-shaped cytoplasmic inclusions), which can be demonstrated by electron microscopy.
-
Differential diagnoses include osteomyelitis, granulomatous inflammation, Hodgkin's and non-Hodgkin's lymphoma.
Identification of morphologic features of Langerhans cells and the use of appropriate markers and/or EM help to
resolve diagnostic problems.
-
Clinical behavior. EG is a benign, self-limited disorder. Progression to systemic disease occurs
exclusively in the first two years of life.
Available publications for the topic:
Eosinophilic Granuloma
|

