|
|
Introductory Course
- Welcome to our Bone Tumor Pathology site
- Approach to Bone Tumor diagnosis - Back to Basics
- General considerations
- Relevant clinical information
- Radiological correlation
- General histologic assessment of the lesion.
|
|
|
Welcome to our Bone Tumor Pathology site
Bone tumors represent a unique group of pathologic conditions for which little time is assigned during the
training period in most Pathology residency programs.
This website is created to introduce trainees in Pathology to the basic concepts in diagnosis of bone tumors.
It is structured to walk you through this difficult field in a stepwise manner by which you will familiarize yourself with
the various common skeletal tumors and tumor-like conditions.
At this site you will find:
- Overview of clinical, radiological and pathologic findings, characteristic of common bone tumors
- Case studies with relevant radiological and pathologic images
- Learn the importance and application of a combined clinico-radiologic-pathologic approach to Bone Tumor diagnosis.
Due to the limitations posed by the format of an online tutorial, the lesions discussed here are only those
that are most common, and those that may present serious diagnostic difficulties. Obviously, the site is not meant
to be all-inclusive and only serves a simple purpose of getting you started. For detailed information we would
refer you to the following texts, which were used as sources for this website:
- Dorfman HD, Czerniak B: Bone Tumors. Mosby, Inc.1998
- Helliwell TR: Pathology of Bone and Joint Neoplasms. Philadelphia, WB Saunders Co.1999
- Mirra JM: Bone Tumors: Clinical, Radiologic and Pathologic Correlations. Philadelphia, Lea & Febiger 1989
- Fechner RE, Mills SE: Tumors of the Bones and Joints. Washington, DC: Armed Forces Institute of Pathology; 1993. Atlas of Tumor Pathology; 3rd series, No.8
- McCarthy EF, Frassica FJ: Pathology of Bone and Joint Diseases. Philadelphia, WB Saunders Co. 1998
- Unni KK(ed): Dahlin's Bone Tumors, 5th ed. Philadelphia, Lippincott-Raven 1996
Please read through the Introductory Course before moving on to the Case Studies section. Unknown Slides section (quiz) is available if you wish to test your knowledge. There is also a Search option, if you need to look up a specific entity.
We are glad to have you here, and we would appreciate your comments and suggestions. Good luck!
|
|
|
Approach to Bone Tumor Diagnosis
General Considerations:
Bone Tumors can be divided into primary and secondary. Secondary tumors can be further subdivided into
- Metastatic tumors
- Tumors resulting from contiguous spread of adjacent soft tissue neoplasms
- Tumors representing malignant transformation of the pre-existing benign lesions.
Metastatic cancers are the most frequent malignant tumors found in bone.
They are by far more common than primary bone tumors and are characterized by the following:
- Predominant occurrence in two age groups: adults over 40 years of age and children in
the first decade of life.
- Multifocality and predilection for the hematopoietic marrow sites in the axial skeleton
(vertebrae, pelvis, ribs and cranium) and proximal long bones. Metastases to long bones
distal to the elbows and knees are unusual. Metastases to the small bones of the hands
and feet are even rarer. Occasionally, metastases may appear as solitary lesions
(particularly true for the lung, kidney and thyroid cancer).
|
|
Most common malignancies producing skeletal metastases:
|
| Adults
|
More than 75% of skeletal metastases originate from carcinomas of the prostate,
breast, kidney, and lung. Also common are metastases from thyroid and colon cancers. And
do not forget melanoma.
|
| Children
|
Neuroblastoma, rhabdomyosarcoma, and retinoblastoma
|
|
|
Radiographic appearance of the metastatic tumors can be
|
|
|
-Purely lytic (kidney, lung, colon, and melanoma)
-Purely blastic (prostate and breast carcinoma)
-Mixed lytic and blastic (most common appearance)
|
|
Primary bone tumors are characterized by the following:
- Predominant occurrence in the first 3 decades of life,
during the ages of the greatest skeletal growth activity. The commonest sites for many
primary tumors, both benign and malignant, are in the distal femur and proximal tibia,
the bones with the highest growth rate.
- Relatively specific radiographic presentations. In some cases, the diagnosis can be
confidently made based on the radiographic features alone.
- Benign tumors are by far more common than malignant ones. Some of them are not true
neoplasms, but rather represent hamartomas (eg., osteochondroma). The most
common benign tumors are osteochondroma, non-ossifying fibroma, and enchondroma.
- Some primary bone tumors are difficult to classify as benign or malignant. For example,
giant cell tumor of bone is very aggressive locally but only rarely metastasizes.
- Among primary malignant neoplasms, osteosarcoma and multiple myeloma have the highest
incidence, followed by chondrosarcoma and Ewing's sarcoma.
Two important features of bone tumors:
- The ability of some to dedifferentiate (eg., enchondroma or a low-grade chondrosarcoma transforming into
a high-grade sarcoma)
- Tendency of high-grade sarcomas to arise in damaged bone, at the
sites of bone infarcts, radiation osteitis and Paget's disease.
|
|
|
Relevant clinical information
|
|
AGE (probably the most important clinical clue).
|
|
Age group
|
Most common benign lesions
|
Most common malignant tumors
|
|
0 - 10
|
simple bone cyst
eosinophilic granuloma
|
Ewing's sarcoma
leukemic involvement
metastatic neuroblastoma
|
|
10 - 20
|
non-ossifying fibroma
fibrous dysplasia
simple bone cyst
aneurysmal bone cyst
osteochondroma (exostosis)
osteoid osteoma
osteoblastoma
chondroblastoma
chondromyxoid fibroma
|
osteosarcoma,
Ewing's sarcoma,
adamantinoma
|
|
20 - 40
|
enchondroma
giant cell tumor
|
chondrosarcoma
|
|
40 & above
|
osteoma
|
metastatic tumors
myeloma
leukemic involvement
chondrosarcoma
osteosarcoma (Paget's associated)
MFH
chordoma
|
|
|
|
|
Summary: Primary osteosarcoma and Ewing's sarcoma are tumors
of children and young adults. Occurrence of chondrosarcomas in children or Ewing's sarcoma
in middle-aged patients is extremely unusual. In individuals older than 40 years,
the commonest form of skeletal malignancy is metastatic cancer. Of the primary bone tumors
in this age group, multiple myeloma and chondrosarcoma are most commonly encountered.
Osteosarcomas in this age group are often secondary malignancies, which develop at the
the sites of bone damage. Giant cell tumor, a locally aggressive lesion, almost exclusively occurs in skeletally
mature patients, 20 to 50 years of age, with closed epiphyses. It is practically never seen
in children or patients older than 60 years.
|
|
|
PAIN (although a non-specific symptom, it may help in differential diagnosis).
Generally, benign non-growing lesions tend to be asymptomatic and represent incidental
findings. Pain may be a symptom of:
- Growing lesions. This category includes locally aggressive lesions
(eg., aggressive osteoblastoma and GCT), and malignant tumors
- Pathologic fracture complicating either benign or malignant tumor
- Significant local tissue reaction to the tumor.
The following clinical symptoms are worth remembering since they may help in the
differential diagnosis:
- Osteoid osteoma - small lesion, but highly irritative to adjacent tissues
and typically causes intense night pain relieved by non-steroidal anti-inflammatory drugs.
Osteoid osteomas may also occur close to the articular surface of a joint, causing
severe inflammatory synovitis, which often obscures the presence of the tumor.
- Enchondroma vs. chondrosarcoma, grade 1 - histologically, the distinction
between a grade 1 chondrosarcoma and an enchondroma is extremely difficult, as histologic
features overlap considerably. The distinction is based on the behavior of the lesion.
One of the clues to clinical behavior is the presence of pain. Low-grade chondrosarcoma
is a growing tumor and, therefore, presents with pain. Enchondromas tend to be asymptomatic,
unless associated with a pathologic fracture.
|
|
|
|
MULTIPLE LESIONS Although both benign and malignant tumors may be
multifocal, benign lesions tend to show symmetrical distribution.
|
|
|
Radiological Correlation
|
The following imaging studies are commonly used in evaluation of bone tumors:
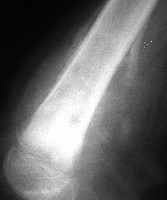
PLAIN RADIOGRAPH is usually the first imaging technique for a suspected bone lesion
since it is inexpensive and easily obtainable. It is also the best for assessment of general
radiological features of the tumor.
COMPUTER TOMOGRAPHY is a method of choice when plain film assessment is difficult owing
to the nature of the lesion (eg., permeative pattern of destruction) or anatomic site
(eg., sacrum). In addition, CT is the best technique in assessment of matrix mineralization,
cortical detail, and detection of the cystic and fatty lesions.
MRI is a method of choice for local staging. It is superior to CT in the definition
of medullary and extracortical spread and of the relationship of the tumor to critical
neurovascular structures. However, remember that the MRI appearances of the majority of
bone tumors are totally non-specific. You need to examine plain films or CT films to define a
neoplasm.
BONE SCINTIGRAPHY is a highly sensitive but relatively non-specific technique.
Its main role is in detection of suspected metastases in the whole skeleton. It may also be
helpful in the detection of osteoid osteomas ("double density sign" is present in about
50% of cases and is highly suggestive of this tumor).
|
Radiographic examination should answer the following questions:
- What is the precise location of the lesion (type of bone and, if the long bone is affected, where exactly the lesion is centered - cortex or medulla; epiphysis, metaphysis or diaphysis)? Some tumors almost exclusively occur at specific sites; many oth
ers favor certain locations.
- Is there any evidence of underlying bone abnormality (eg., bone infarct, Paget's disease)? High-grade sarcomas tend to arise in damaged bone.
- Is the lesion multifocal?
- Does the tumor have a well-defined margin? Is there a rim of sclerotic bone? The presence of a well-defined margin and a sclerotic rim strongly suggests a benign non-growing lesion.
- Is there evidence of significant cortical expansion or destruction? These findings are seen with locally aggressive or malignant tumors.
- Is there an associated periosteal reaction and, if so, of what type? See discussion below.
- Does the lesion produce mineralized matrix (osteoid or cartilage)?
- Is there a soft tissue mass?
In many cases, the radiographic appearance of the lesion provides clues to its clinical
behavior. It allows estimation of tumor growth rate and discloses expansive or
infiltrative growth patterns characteristic of locally aggressive and malignant
tumors.
|
|
|
SKELETAL LOCATION (while many lesions favor certain bones, some tumors
almost exclusively occur at specific sites)
|
Lesions
|
Most common skeletal sites
|
Ewing's sarcoma
Multiple myeloma
Leukemia/lymphoma
Metastatic cancers
|
Hematopoietic marrow sites in the axial skeleton
(vertebrae, ribs, sternum, pelvis, cranium) and proximal
long bones (femur, humerus)
|
|
Non-ossifying fibroma
|
Metadiaphyseal regions of the tibia and distal femur (80%)
Does not occur in the flat bones, craniofacial bones, the spine, or the small
bones of the hands/feet.
|
|
Simple bone cyst
|
The vast majority of SBCs is found in the proximal humerus (55%) and proximal femur (20%).
|
|
Chordoma
|
Base of the skull or sacrum (90%)
|
|
Adamantinoma
|
Mid-shaft of tibia (90%), jaw bones
|
|
Chondroblastoma
|
Long bones (knee area, proximal humerus)-70%
|
|
Giant cell tumor
|
Knee area, distal radius (65%)
|
|
Enchondroma
|
Small bones of the hands and feet (60%). This is in fact the commonest tumor at these sites.
|
|
Chondrosarcoma (primary, and to the less extent secondary)
|
Tends to develop in the axial skeleton with 25% to 30% occurring in the pelvic bones
|
|
Fibrous dysplasia
|
Femur, tibia, skull and ribs
|
|
Osteochondroma
|
Knee area, proximal humerus, pelvis
|
|
Osteoblastoma
|
Spine (30%), mandible, long bones
|
|
Aneurysmal bone cyst
|
Any bone; common in the spine
|
|
Chondromyxoid fibroma
|
Knee area (30%), pelvis, small bones of the feet
|
|
Hemangioma
|
Spine, craniofacial bones
|
|
|
|
SITE OF LONG BONE INVOLVEMENT
(most primary bone tumors have favored sites within long bones; this may provide a clue to diagnosis).
|
|